As an Orthopaedic Doctor this is something I help patients manage. Knee pain can develop at any time, ranging from young adults to older people.
Usually the age at which you experience knee pain, fits into a loose pattern
Younger age (under 50 years): Sports injury or trauma related, meniscal injuries, patella dislocation, early osteoarthritis, juvenile arthritis, developmental disorder of the knee, radiating pain (from hip or ankle), quadricep or patella tendinopathy
Middle age (50 – 70 years): early Osteoarthritis, sequelae of trauma (tibial plateau fractures) or knee conditions, Spontaneous osteonecrosis of the knee (SONK), radiating pain (from hip or ankle), quadricep or patella tendinopathy
Older age (above 70 years): sequelae of trauma, Osteoarthritis, radiating pain (from spine or knee), quadricep or patella tendinopathy
Are you looking for treatment of Knee pain or Knee replacement?
You may have seen or tried alternative treatments. This could range from analgesia (pain killers), optimising medical conditions (diabetes, heart disease, chest/ lung conditions), walking aids, losing weight, physiotherapy, injection therapies (Platelet rich plasma (PRP), Ostenil (hyaluronic acid) or steroid/ cortisone), knee arthroscopy (keyhole Procedure) or knee replacement Procedure.
Symptoms: You may experience pain at various times in the day, but particularly what patients mention is pain at night and difficulty either getting to sleep or staying asleep. It can result in a significantly disturbed sleep which can have an impact on your next day. Another symptom is stiffness, this can be particularly exacerbated when you wake up in the morning and go to stand up from a seated position. It can take you a few steps before your joint starts to lubricate itself and you can get moving. It can even happen when you have been seated for any length of time and you go to stand, you can find yourself taking a few hobbling steps before you start walking normally.
Analgesia (pain killers) for knee pain: These can range from simple pain relief such as Paracetamol (provided you have no contraindications) and Ibuprofen (provided you have no contraindications), following the World Health Organisation’s ladder of pain.
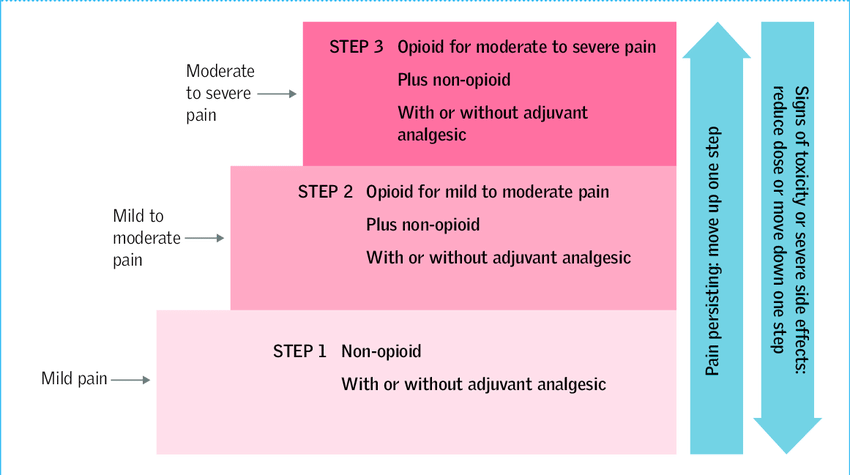
Your General physician will then guide you to stronger analgesia (pain killers) such as codeine, tramadol and then different formulations of morphine. You can also enquire about Fentanyl patches which can be particularly effective in some people.
Some patients may also find topical gels such as Ibuprofen or diclofenac, when used sparingly to also help them with their pain. You may also find a heat pad (to be used as directed by manufacturer) on the joint for short intervals to also provide some relief. That is why some people find their knee pain can improve in warmer climates.
 Optimising medical conditions: If you suffer from conditions such as Diabetes, Heart disease, Lung conditions, Rheumatoid or Inflammatory conditions such as Lupus, Polymyalgia rheumatica or Psoriasis may have an impact on your joint pain. This can result from a combination of muscular weakness, generalised pain or generalised inflammation. For diabetes one should always look to optimise your blood sugars as too low or too high can have an impact on your health.
Optimising medical conditions: If you suffer from conditions such as Diabetes, Heart disease, Lung conditions, Rheumatoid or Inflammatory conditions such as Lupus, Polymyalgia rheumatica or Psoriasis may have an impact on your joint pain. This can result from a combination of muscular weakness, generalised pain or generalised inflammation. For diabetes one should always look to optimise your blood sugars as too low or too high can have an impact on your health.
Walking aids: These have been proven to reduce the joint reaction force acting on the knee joint. This works by offloading the knee joint and transferring the weight/ force through the walking stick instead of the knee joint. Sometimes some people find a walking stick is not for them for a variety of reasons (end up with a painful wrist or hand, don’t like the look of them, etc), therefore one can use an elbow crutch as it can provide more support to your arm. I have also realised over time that some patients prefer walking poles, utilising either one or two as per preference.
Orthotics: insoles can also help if you suffer from flat feet which could put pressure on the knee joint. More importantly if you have a problem with the knee on one side, I have noticed that it can have a detrimental effect on the opposite hip. So if there is a problem you may benefit from treatment of the hip symptoms, which may improve your knee symptoms. This usually happens as your knee is trying to compensate for the opposite hip, in order for you to walk normally.

Losing weight to reduce knee pain: This is one aspect that is in your control and people who are overweight must consider. This is a simple analogy of the suspension of your car (similar to the joints in your body), if it was being overloaded you would empty the load in the boot/ trunk. This translates into reducing the extra weight which you may be carrying around. Now there are various modalities to reduce your weight ranging from dieting to bariatric Procedure. What is best for you is to calculate your BMI and see where you are on the scale. Then decide if you want to do it alone or do you need support. The key ingredient is will power. I have had patients join various self-help courses, weight loss clubs and have also referred to our specialist endocrine unit based at Salford Royal NHS Foundation Trust.
Some people who may be overweight may in fact be malnourished, as they may not be consuming the right nutrients for themselves.
Exercise and Physio: Depending on the condition being treated, physiotherapy is accordingly targeted. This can focus on strengthening the quadricep and calf muscles to reduce the load on the knee joint itself. The knee joint is the largest joint in our body which relies on the tone of your muscle to maintain its stability. So if you proceed with physiotherapy diligently you may find your knee symptoms improve drastically. Hydrotherapy can also be very effective in controlling knee pain. Our joints are designed to move, hence simple exercise such as walking up to 30 minutes per day can improve your wellbeing and your health.
Do you need help with your knee pain?
Call us on 01625 529942 or Book a consultation
Injection therapies: Over the years I have perfected identifying the correct injection therapy for patients and injecting technique. Depending on the extent of your hip pain I will recommend which injection therapy accordingly. This can range from PRP (platelet rich plasma) injections, which is usually a course of 3, one injection every 1-2 weeks. This I usually utilise for patients with early or moderate changes in their knee joint, it can also be very effective in sports injuries.
The next injection therapy I may recommend is Ostenil, which is a synthetic hyaluronic acid which is a substance naturally produced by the body. I find it best utilised in patients with early to moderate degenerative changes in their joints.
I reserve the use of steroid (cortisone) injection in the joint until there is moderate to severe degenerative changes in the joint.
The outcomes from injections can be extremely variable, where some injections last from a few weeks to over year! It can be however a very effective treatment to overcome the most debilitating symptoms which is pain, especially in the short term. There are risks involved with any type of therapy and these will need to be discussed with you by your physician or orthopaedic doctor.
Knee arthroscopy: In my opinion this has a specific role in the management of knee pain. This is usually for patients with an identifiable problem within the articulation of the hip joint. This can be related to mechanical symptoms such as the knee giving way or locking in a position. This can be due to pain, meniscal or cartilage injuries.
Knee replacement Procedure: This has been reported as one of the main break throughs in medicine and has been proven as one of the best operations to improve the quality of life of patients.
It is essentially indicated if you have significant painful symptoms as it is primarily a pain-relieving procedure. In my opinion I believe it can also improve your function as, once you remove the painful stimulus from the knee, it should move better, hence allowing you to walk again pain-free and even run in some instances. I do not recommend jogging however as the jarring motion can affect the prosthesis. As opposed to walking and running which are smoother movements.
A knee replacement removes the degenerative knee (hinge) joint and replaces it with an artificial joint. The two prostheses (what are implanted into your body – one at the end of your thigh (femur bone) and one on top of the shin (tibia) bone).


The prosthesis can either be cemented into position or be uncemented. I will provide a bespoke solution after discussing with you the pros and cons of each.
This procedure was refined to what it is today by Sir John Charnley and I am proud to say that I am one of the last Charnley fellows to have been trained at Wrightington hospital where he himself worked and carried out his pioneering work.
What if I can’t have knee replacement Procedure?
In my practice I occasionally come across patients who are not suitable or are unable to have Procedure due to their medical conditions being significant or their weight may be prohibitive to Procedure. In these very small number of cases we do explore the possibility of nerve ablation therapy. This carried out in partnership with one of my Pain consultants. They firstly anaesthetise the nerves in turn to identify the ones which are causing the pain. Once identified those specific nerves are targeted and ablated.
Can your knee pain get better?
YES…provided we identify the source of it.
I therefore ensure that my patients are investigated prior to any treatment being advocated so we address the source of the problem and not just the symptoms.
If you have been suffering with knee pain then you may have already looked at different options to help yourself. Some of these alternative treatments for hip pain include: Glucosamine or Turmeric tablets, various gels like Flexiseq and also some other remedies. Unfortunately, we do not have any evidence in the medical literature to advise us whether or not these treatments are helpful or not.
If you are looking for an orthopedic Doctor and knee replacement specialist in Cheshire, Stockport and Manchester area, do not hesitate to give us a call on 01625 529942 or book a consultation here at Canova Medical in Wilmslow.